
Fifty years ago, President Lyndon Johnson began his quest for a more just and honorable America with the passage of the Civil Rights Act of 1964, passed the Voting Rights Act of 1965 and the Fair Housing Act of 1968. This week, President Barack Obama joined three former Presidents delivered remarks at the Civil Rights Summit at the Lyndon B. Johnson Presidential Library and Museum, and acknowledged racism has hardly been erased and that government programs have not always succeeded. Let us talk about socioeconomic and racial/ethnic disparity patterns in public health. What the patterns tell us? In Europe, the presence of detailed socioeconomic information in routine health data has facilitated the monitoring of socioeconomic patterns in diverse health indicators (Braveman, Cubbin, Egerter, Williams & Pamuk, 2010). This socioeconomic information gave Public health professionals and researchers the ability to compare health of socioeconomically disadvantaged population with health differences among middle-class subgroups and, potentially, comparisons with the wealthy. Braveman et al. (2010) gave emphasis on Europe’s data collection in contrast with routine the routine public health statistics in the United States. Health difference across groups defines by socioeconomic factors have been examined less frequently. It was further noted by the study that routine health reporting should examine socioeconomic and racial/ethnic disparity patterns, jointly and separately. According to Collins (2004) “race and ethnicity are poorly defined terms that serve as flawed surrogates for multiple environmental and genetic factors in disease causation, including ancestral geographic origins, socioeconomic status, education and access to health care. Research must move beyond these weak and imperfect proxy relationships to define the more proximate factors that influence health” (para. 1).
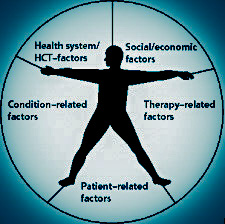
Health disparities in many instances will hardly to do with genetics, but more directly associated in socioeconomic status (SES), access to health care, education, social marginalization, discrimination, culture, stress, diet and other factors. SES is one of the strongest and most consistent predictors of morbidity and mortality. As a complex phenomenon, the impact of SES on disease makes its definition and measurement of vital importance. SES is typically measured by determining education, income, and occupation (Winkleby, Jatulis, Frank & Fortmann, 1992). The Farquhar et al study is the only U.S. study on the associations between separate SES dimensions and risk factors or disease outcomes (Winkleby et al., 1992). In the Farquhar et al. study (1985): Subjects aged 25 to 64 were drawn from the two control cities of the Stanford Five-City Project, a communitywide cardiovascular disease intervention study that contains data from four separate cross-sectional surveys, conducted from 1979 to 1986. Participants who were unemployed (n = 98), students (n = 130), or retirees (n = 146) were excluded because they had no occupation that could be ranked (Winkleby et al., 1992, p. 816). Associations between one measure of SES and one risk factor, morbidity, or mortality in other studies have found that education is more strongly associated with disease than income or occupation. One of the most complete studies of mortality differentials (Kitagawa et al., 1973) found “lower SES groups exhibited higher rates of all-cause mortality than did higher SES groups, irrespective of whether education, income, or occupation was used as the measure of SES” (p. 819). Lower levels of education are associated with hypertension, cigarette smoking, high cholesterol, cardiovascular disease (CVD) morbidity and mortality. According to Winkleby et al., there are no SES measure that is universally valid and suitable for all populations. The study noted “if economics and time dictate that a single parameter be chosen, and if the research hypothesis does not dictate otherwise, the conclusion is that higher education, rather than income or occupation, may be the strongest and most consistent predictor of good health” (p. 819).
References
Abramson, J., Gofin, R., Habib, J., Pridan, H. & Gofin, J. (1982). A comparative Appraisal of measures for use in epidemiological studies. Soc Sci Med., 16,1739-1746.
Berger, M. & Leigh, J. (1989). Schooling, self-selection and health. J Hum Res. 24, 433-455.
Civil Rights Summit. (n.d.). Retrieved from http://www.civilrightssummit.org/ Chicago: Civil Rights Summit, http://www.civilrightssummit.org/ (accessed April 12, 2014).
Dyer, A., Stamler, J., Shekelle, R. & Schoenberger, J. (1976). The relationship of education to blood pressure: findings on 40,000 employed Chicagoans. Circulation. 54, 987-992.
Helmert, U., Herman, B., Joeckel, K., Greiser, E. & Madans, J. (1989). Social class and risk factors for coronary heart disease in the Federal Republic of Germany: results of the baseline survey of the German Cardiovascular Prevention Study. J Epidemiology Community Health. 43, 37-42.
Hypertension Detection and Follow-up Program Cooperative Group. Race, education and prevalence of hypertension. (1977). Am J Epidemiology. 106, 351-361.
Jacobsen, B. & Thelle, D. (1988). Risk Factors for coronary heart disease and level of eduvation. Am J Epidemiology. 127, 923-932.
Kitagawa, E. & Hauser, P. (1973). Differential mortality in the United States: Study in socioeconomic epidemiology. Harvard University Press, Cambridge, Mass.
Labilles, U. (2013). What the Patterns Tell Us: Socioeconomic Status and Health (Unpublished, PUBH 8115-1 Wk6 Discussion, Social Behavioral and Cultural Fact in Public Health Spring Qtr.) Walden University, Minneapolis.
Millar, W. & Wigle, D. (1986). Socioeconomic disparities in risk factors for cardiovascular disease. Can Med Assoc J. 134, 127-132
Matthews, K., Kelsey, S., Meilahn, E., Kuller, L. & Wing, R.(1989). Educational attainment and behavioral and biological risk factors for coronary heart disease in middle-aged women. Am J Epidemiology, 129, 1132-1144.
Socioeconomic status and health: … preview & related info … (n.d.). Retrieved from http://www.mendeley.com/catalog/socioeconomic-status-health-education-income-occupation-contribute-risk-factors-cardiovascular-disea/
Socioeconomic disparities in health in the United States … (n.d.). Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/20147693
Pinsky, J., Leaverton, P. & Stokes, J. (1987). Predictors of good function: The Framingham study. Journal of Chronic Disease, 40, 159S-167S.
Snowden, D., Ostwald, S. & Kane, R. (1989). Education, survival and independence in elderly Catholic sisters. American Journal of Epidemiology, 130, 999-1012.
What we do and don’t know about ‘race’, ‘ethnicity’, genetics … (n.d.). Retrieved from http://www.nature.com/index.html?file=/ng/journal/v36/n11s/full/ng1436.html
